Academic (research and teaching) vision for the next five years
My vision for the next 5 years is to complete PgCAP and become a fellow of the HEA. On completion I hope to obtain a permanent lecturing contract with the University of Edinburgh. To further support my application for a lecturing position, I wish to embark on research project or an MSc concerning BSc Oral Health Sciences (OHS) student diversity. I have a particular interest in the educational background of students who embark on the course and the factors that affect their success within the discipline. I would hope that this research could be utilised to target and support students and reduce dropout rates.
Teaching and Research Objectives
In 2016 I was appointed as a lecturer for BSc OHS on a secondment basis. Since then I have had opportunity to teach in a variety of mediums; “traditional” lecturing transmission of information (Åkerlind, 2004), clinical practical skills development, and clinical patient supervision. Students generally engage well in the practical aspects of the curriculum highlighted in the BSc (Hons) OHS Student Midterm feedback (Y1-3):
“helps build confidence” and “closely resembles treatment you will carry out”.
However, in other theoretically heavy “threshold concepts” (Cousin, 2006) such as Health and Disease, students reported;
“Overwhelming amount of information” and requested “more interactive lectures” such as “short quizzes”.
One of my teaching objectives is to introduce different techniques for knowledge transfer in the theoretical concepts of the discipline.
An estimated 30% of my teaching time is occupied supervising students on patient clinics. Feedback is given privately to students for each appointment immediately following completion. My next teaching objective is to further improve my formative feedback skills to ensure that students have specific and achievable targets to strive towards.
During my undergraduate studies academic writing opportunities were limited due to the absence of an honours year. I now want to develop my skills writing at an academic level to enable myself to provide high quality support to my undergraduate students. When advising students on their dissertations and literature reviews, I often consult colleagues for advice on my summative feedback as they are more experienced. I hope that as my experience of writing assignments for PgCAP progress, I will need to rely less on my colleagues for continual support.
Boyd and Smith state that;
“the majority of university lecturers in the health professions have been appointed on the basis of their successful first career in clinical practice” and that have “little or no direct experience of involvement in research activity” (2016).
I agree with this statement following the PgCAP orientation days where I met many academics working in other disciplines who demonstrate vast experience in research. Therefore, my objective is to embark on collaborative research with colleagues in my discipline to examine student diversity issues within BSc OHS and resulting employment as Dental Care Professionals.
This year I have been appointed as Personal Tutor to 2017-2018 Y1 BSc OHS. During the last academic year, a significant number of our students embarked on the appeal process. This lead the discipline to reflect on the standards of our Euclid notes and how we approach student’s academic and personal issues. We are fortunate to have very small cohorts of students, improving our ability to recognise quickly when issues arise. My objective is to better understand what students require from their PT and how best to carry out these duties from the pastoral and counselling services available.
Campaign plan for achieving these objectives
In response to student feedback, my campaign plan includes the implementation of newly researched knowledge transfer techniques such as Top Hat (Galloway, 2017), Qwectures and flipped lectures (McQueen, 2016). I will continue to attend IAD development courses and utilise the teaching matters blog for advice and examples of these techniques in action. I will share successful techniques with my team to collectively improve student engagement, thus making my colleagues key beneficiaries within my plan.
Particular to Oral Health Sciences, I hope to utilise available resources of 3D anatomy suite and the video camera in clinical skills to improve student engagement in this curriculum area. To achieve this, I will allocate protected time to receive training on use of these technical facilities. Last semester, I trialled a restorative handbook for semester one of Y2. From experience of the previous academic cycle, I noticed gaps in continuity and uniformity when teaching students restorative skills. The handbook contains diagrams, examples, tasks and lectures that are delivered throughout the semester. I included space for students to reflect on each session within clinical skills, however I rarely witnessed this being utilised. My campaign plan is to obtain feedback from colleagues and students on how to improve the handbook efficiency. Personally, I have already identified the need for lecturers to give formative written feedback on tasks carried out, which may in turn encourage students to utilise the space for reflection.
Regarding formative feedback, I plan to develop a template for this on clinics. Feedback is currently given verbally by the supervisor and is recorded by the student. The supervisor must electronically sign off the reflective account but there is only room for comment if a low grade has been given. When I think back to my undergraduate training, I valued direction and used it to improve, however positive comments were verbal and rarely recorded. Allowing the supervisor to add comment, regardless of the grade outcome, may support those students who often feel they are only ever given critical feedback.
I recently met with my personal tutor for PgCAP to discuss the optional courses. I greatly appreciated the advice and guidance given and have chosen the optional course “Researching your teaching” where I hope to develop my research skills. The course assignment is to write a research proposal, which I intend to be in dental education and student diversity. I will seek advice from colleagues who have completed their masters on how to relate my research proposal to the discipline. I hope there may be potential opportunities for collaboration on a research project with my colleagues, post PgCAP completion.
Identification of key beneficiaries, collaborators and partners
In no hierarchical order, the key beneficiaries within my plan are the discipline, colleagues, students and myself.
I anticipate that BSc OHS will benefit through on going course development and ensuring lecture content continues to be in line with current advances in dentistry and teaching techniques. Colleagues will benefit from the sharing of acquired knowledge from PgCAP and collaborative opportunities that may arise when I embark on dental education research.
Conceivably the most important beneficiaries of my personal plan are the undergraduate students within the course. Evidence of course adaptations made in response to student feedback, will ensure students feel their input is valued and encourage an “ethos of respect” (Kreber, 2010). Through improvements in teaching styles using the technology previously mentioned, verbatim “mimicry” (Cousin, 2006) of lecture content by students should decline, as they demonstrate a deeper level of understanding. Students often express stressed emotions regarding coping with discipline content especially before examinations. Through further PT training and collaboration with colleagues, I will be better equipped to assist and support students in need of academic and personal guidance at these times.
Personally, I feel I will benefit from the opportunity to begin building my academic identity (Kreber, 2010) and reputation within dental education. I have entered a post in academia relatively early in my career and plan to utilise PgCAP as an opportunity for further academic development.
Key challenges, opportunities and funding
September 2020 is the expected completion date of my secondment. I am fortunate to have the opportunity to complete PgCAP during this time frame however, I expect that the progression of research may extend beyond this date.
Development of the course content is necessary and continuous as the discipline is governed by the General Dental Council (GDC) standards framework. Curriculum is set by the GDC and must be accurately taught, currently by traditional lectures. When adopting new teaching methods, the challenge is to ensure accuracy of information students receive whilst encouraging them to further their learning through independent research.
UKPSF Framework Dimensions covered – K4, K5, V1, V3, V4
References
ÅKERLIND, S. (2004) A new dimension to understanding university teaching. Teaching in Higher Education. 9:3, pages 363-375. [online]. Available from: https://doi.org/10.1080/1356251042000216679 [Accessed: 07 Dec 2017]
BOYD, P., SMITH, C. (2016) The contemporary academic: orientation towards research work and researcher identity of higher education lecturers in the health professions. Studies in Higher Education. 41:4, pages 678-695. [online]. Available from: https://doi.org/10.1080/03075079.2014.943657 [Accessed: 07 Dec 2017]
COUSIN, G. (2006) An introduction to threshold concepts. Planet. 17:1, 4-5, pages 4-5. [online]. Available from: http://www.tandfonline.com/doi/pdf/10.11120/plan.2006.00170004?needAccess=true [Accessed: 14 Dec 2017]
GALLOWAY, R. (2017) Teaching Matters blog [online]. The University of Edinburgh. Available from: http://www.teaching-matters-blog.ed.ac.uk/?p=1533 [Accessed: 19 Dec 2017]
KREBER, C. (2010) Academics’ teacher identities, authenticity and pedagogy. Studies in Higher Education. 35:2, pages 171-194. [online]. Available from: https://doi.org/10.1080/03075070902953058 [Accessed: 06 Dec 2017]
McQUEEN, H. (2016) Teaching Matters blog [online]. The University of Edinburgh. Available from: http://www.teaching-matters-blog.ed.ac.uk/?p=888 [Accessed: 19 Dec 2017]
Further Reading
BOMBERG, E. (2016) Teaching Matters blog [online]. The University of Edinburgh. Available from: http://www.teaching-matters-blog.ed.ac.uk/?p=198 [Accessed 06 Dec 2017]
BREW, A. (2010) Imperatives and challenges in integrating teaching and research. Higher Education Research & Development. 29:2, pages 139-150. [online]. Available from: https://doi.org/10.1080/07294360903552451 [Accessed: 07 Dec 2017]


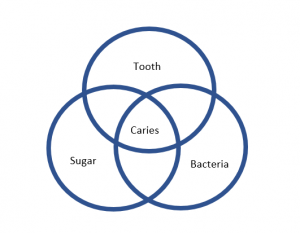 ng or continuing to progress. Once students understand this relatively straightforward concept they can research any of these factors such as species of bacteria, and diet advice for minimising sugar intake. The further research will aid students with patient education which is integral task in their role as Dental Care Professional.
ng or continuing to progress. Once students understand this relatively straightforward concept they can research any of these factors such as species of bacteria, and diet advice for minimising sugar intake. The further research will aid students with patient education which is integral task in their role as Dental Care Professional.